Starting in World War I, military hospitals moved closer and closer to bullets-flying combat, culminating in the legendary Korean War MASH units.
Two years before the United States declared war on Germany, in 1915, a few American physicians were already in Europe, caring for the gassed and wounded soldiers streaming into Paris from the trenches of France. The physicians were volunteers in the Ambulance) Hospital, and many were Ambulance Américaine (American distinguished surgeons on three-month rotations from the faculties of American medical schools. Among them were Dr.George Washington Crile, who, as a professor of surgery at Western Reserve School of Medicine, had pioneered the use of person-to-person blood transfusions during surgery; and Dr. Harvey Williams Cushing of Harvard Medical School, a world-famous neurosurgeon whose specialty was saving soldiers by opening their skulls and plucking out shrapnel without harming their brains.
Crile and Cushing, convinced that the United States would soon be at war, came home with a bold idea: transform American medical schools and leading civilian hospitals into wartime military hospitals. Major General William C. Gorgas, the army surgeon general, enthusiastically welcomed the idea, and by the time the United States entered the war, it had been implemented. Over several decades and several wars, Crile and Cushing’s original concept mutated into something far different—Mobile Army Surgical Hospitals. In the Korean conflict, these MASH units were close to the front and staffed by civilian doctors who broke the rules—one Army Medical Corps historian described them as “professional doctors but amateur soldiers.” They were later portrayed as irreverent surgeons Hawkeye and Trapper John in the highly popular M*A*S*H* television series (1972–1983). The show’s grimly hilarious scenarios reflected what could happen when cool civilian surgeons were plunged into the cauldron of war.
The long trail from Ambulance Américaine to MASH begins with Surgeon General Gorgas, who immediately saw the advantage of injecting civilians into the Army Medical Corps. Gorgas had become famous in 1905 for leading a controversial crusade to wipe out disease-carrying mosquitoes that were debilitating the workers building the Panama Canal. His renown helped him as he led the campus-to-combat idea through the barricades of longstanding army doctrine. Gorgas reached out to physicians and nurses at medical schools and hospitals. Under his plan, the civilians, already accustomed to working together, would form the staffs of what the army called Red Cross hospitals, after the institution that raised the funds to equip them. As Gorgas envisioned the conversion and mobilization, each hospital would be militarized with an army commanding officer and staff, along with a sergeant major and a cadre of enlisted men who would serve as orderlies and perform nonmedical duties. The physicians would be given commissions, but the nurses would serve without rank as Red Cross nurses. It was a deft way to handle, among other things, Red Cross involvement. If war came, the civilians would be given basic training—from saluting to setting up tents—at U.S. bases and then sent overseas as needed.
Universities enthusiastically mustered staffs drawn from the faculties, students, and alumni of their medical schools, while the Red Cross recruited physicians from major civilian hospitals. Each of these staffs would serve in what the army designated as a base or field hospital beyond the sound of guns. By the time the United States declared war on April 6, 1917, there were 33 Red Cross hospital staffs ready for war, including Dr. Crile’s Base Hospital No. 4 from Western Reserve and Dr. Cushing’s Base Hospital No. 5 from Harvard. Crile’s No. 4, the first U.S. army unit to arrive in France, reached there ahead of General John J. Pershing, commander of the American Expeditionary Forces. The Red Cross’s swift deployment of its “hospitals” displeased army general staff officers, who had heard little about these civilian-type hospitals and did not know how they would fit in with the AEF.
Crile’s No. 4 hospital and other early arrivals were sent to British Army hospitals, replacing physicians who had been killed or wounded. Some American physicians, particularly surgeons, went to British casualty stations at the front. No. 4 stayed with the British Expeditionary Force throughout the war, ultimately caring for 82,179 wounded.
The Red Cross base hospitals took over schools, hotels, villas, and government buildings scattered across France. Base Hospital No. 20, from the University of Pennsylvania, for instance, was sent to Châtel-Guyon, a health resort in the Auvergne Mountains of central France. Eventually, No. 20 became a 2,500-bed hospital spread across 33 buildings. More than 9,000 wounded or gassed soldiers were cared for in the hospital and all but 65 survived. Cushing’s Base Hospital No. 5 was sent to Camiers, site of a major British Army base. No. 5 was bombed during a German night air raid in September 1917, killing an officer and several enlisted men, believed to be the first AEF men killed by enemy action.
As the AEF grew to nearly two million men, the U.S. Army Medical Corps created a complex network that included hospital trains, horse-drawn wagons, fleets of ambulances, battalion aid stations, and hospitals. Many doctors and enlisted men were rotated between base hospitals and a new type of unit—mobile hospitals that brought surgeons close to the front.
The Medical Corps had entered World War I with doctrines formed in the Civil War, and it was proud of the successful adaptations made in France. Of the 224,089 servicemen wounded in that war, 13,691 died of their wounds. More than a million were treated for nonbattle injuries and diseases, especially influenza. The 1918 influenza pandemic, which killed an estimated 50 million people or more worldwide, struck down at least 675,000 Americans, including as many as 46,000 servicemen. Despite the disease’s devastating effects, American troops in the Great War experienced the lowest mortality rates of any previous war.
In September 1939 the eruption of war in Europe led President Franklin D. Roosevelt to declare a “state of limited emergency,” and the army’s new surgeon general, Major General James C. Magee, began preparing for war by turning to civilian physicians and nurses. Magee had served with Base Hospital No. 12 in World War I as part of the Northwestern University Medical School team, and now he revived No. 12 and the base hospital idea in general for a new war.
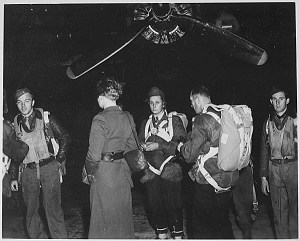
Magee faced problems Gorgas had not known in World War I. Between the wars the army’s medical system had been reorganized, reducing the surgeon general’s power. And the Red Cross would not be raising funds this time for army hospitals, as it had in the previous war. To complicate matters further, old and new doctrines were clashing: While some researchers were developing medical equipment and supplies that could be delivered by parachute, elsewhere in the bureaucracy the purchase of 36 horse-drawn ambulances was being approved. Warehouses were full of obsolete medical equipment and ragged hospital tents, but budget cuts hampered the modernization of the army medical service. “To prepare for war,” said one army history, “the Medical Department had to start almost from scratch.”
Its preparation plan called for the formation of 62 “affiliated units,” again raised by leading hospitals and medical schools but without Red Cross fund-raising. In the spring of 1940, as France was about to fall, Magee began sending out letters, hoping to recruit these affiliated units; many of his letters went to places that had received similar ones two decades before. But this time not all the affiliated units came from medical schools. In October 1940 General George C. Marshall, army chief of staff, was attending a lawn party in Charlotte, North Carolina, when a local surgeon told him that area doctors wanted to organize an affiliated hospital. Marshall explained that medical schools normally sponsored such units, but the doctor persisted. Marshall eventually approved the creation of the 38th Evacuation Hospital, staffed by local physicians and nurses, most from Charlotte Memorial Hospital. Another unit of special origin was General Hospital No. 9, formed in October 1940 by New York Hospital and Cornell University Medical College, formed at the urging of Secretary of War Henry L. Stimson.
Although the staffs of affiliated units completed their army training promptly after being called up, Magee inexplicably kept them at army posts in the United States rather than treating them as the promised rapid-response teams. Twenty affiliated units spent more than a year waiting to go overseas.
Early in the war Magee also changed course, turning against the concept of affiliated unit hospitals and deciding not to create any more, because, he said, the army needed “doctors as individuals, available for assignment when and where they were required.” The doctors, in turn, accustomed to getting their way, appealed to influential alumni and powerful hometown friends. But Magee continued to drain doctors from affiliated unit hospitals by allowing them to volunteer for all-army hospitals.
A former president of the American Medical Association, who was serving as an adviser on army surgery, endorsed Magee’s approach of raiding affiliated units. “We have just got to learn to do the job with what we have,” he said, “and we haven’t enough men to give every hospital a university surgical faculty.” Even No. 9, Secretary of War Stimson’s creation, lost five doctors as Magee volunteers. Each one was rewarded with promotion in rank and appointment as chief of a surgical team in an all-army hospital in a combat zone.
While career army medical officers muttered about the affiliates’ “political and professional cliques” and “old school ties,” they nonetheless wanted such experienced physicians in their hospitals overseas.
Most journeys of the wounded to those lifesaving hospitals began the same way: Medics, unarmed and protected only by red crosses on their helmets, went into the field with a litter or jeep and collected the wounded, carrying them to an aid station 300 yards or so from the front. After what was known as “patch-up work” there, the next stop for most men with serious wounds was a larger hospital, where there were surgeons and new medical miracles: penicillin, sulfa, and blood plasma. Of every 100 wounded men who lived to reach a hospital, 96 survived.
One vocal dissenter to such humanitarian care in combat was Lieutenant General George S. Patton, who had this advice: “If you have two wounded soldiers, one with a gunshot wound of the lung, and another with an arm or leg blown off, you save the son-of-the-bitch with the lung wound and let the goddamn son-of-the-bitch with an amputee arm or leg go to hell. He is no goddamn use to us anymore.”
In order to ensure the best care for the wounded, high-ranking army medical officers joined in combat-logistics planning. The placement of hospitals became a key element in the deployment of troops—and increased the likelihood that wounded men would return to battle. One such hospital, the 70th General, formed by the medical school of St. Louis University, occupied an abandoned Italian army barracks west of Florence. The 70th saved the lives of thousands of soldiers—German, American, and Italian—who were wounded during the long and bloody slog up the Italian peninsula. Among them was Second Lieutenant Robert Dole of the 10th Mountain Division, who arrived in mid-April 1945 as the war in Europe was nearing its end. He had been wounded trying to rescue an American radioman hit by enemy fire when their unit tried to take out a German machine gun nest. Dole’s right shoulder was shattered, neck and spine vertebrae were fractured, and he had shrapnel wounds throughout his body. A week later Second Lieutenant Daniel Inouye of the 442nd Regimental Combat Team, arrived. He had been shot in the stomach and most of his right arm ripped away by a German grenade; the remnants of his arm were amputated. Both men survived and were sent to the same army hospital in Battle Creek, Michigan, where they became acquainted with each other and another wounded soldier, Philip Hart. The three talked about going into politics after the war—and they did, each of them becoming a U.S. senator. (In 2003 the hospital where they met became the Hart-Dole-Inouye Federal Center.)
In Europe 375,000 wounded men left hospitals after treatment and fought again. Overall, death from wounds among U.S. troops in World War II was 3.3 percent, compared to 8.5 percent in World War I. Most medical historians attribute the dramatic drop to the speedy transport of wounded soldiers from frontline patch-up to surgery in the nearest hospital. And eventually the nearest hospital would have the initials MASH.
Early in 1942 Allied strategists had feared that Japan would follow its attack on Pearl Harbor with an invasion of Australia, so medical units were dis- patched there. The first sent was General Hospital No. 4, replaying the fast-moving role of its World War I predecessor. As in Dr. Crile’s Base Hospital No. 4 of that earlier war, most of the doctors in World War II’s No. 4 came from the medical school of Western Reserve University and most of the nurses from the Cleveland area.
Awaiting them was Colonel Percy J. Carroll, chief surgeon of the growing American forces in Australia. As Manila was about to fall to Japanese troops, Carroll had evacuated 224 wounded American and Filipino soldiers and an army nurse, loading them aboard a ship for a perilous voyage to Sydney. Carroll knew that Allied strategists were expecting a long, amphibious Pacific campaign that would be fought across great distances between and on islands of trackless jungles and malarial swamps. And he realized that No. 4 and the three other multi-bed hospitals then on their way to Australia were the wrong kind of hospitals for that kind of war.
He first split the hospitals, designed for 400 to 750 beds, into smaller units. But that was not enough. As he later recalled, he went to his superior—Brigadier General Richard J. Marshall,General Douglas MacArthur’s deputy chief of staff—and said,“I want surgery in the front lines. I want surgery where it’s needed.” Asked what he had in mind, Carroll said, “a portable, surgical hospital.” His idea was rapidly approved, and he headed for General Hospital No. 4, which had taken over a1,000-bed hospital in Melbourne.
After talking about his vision with members of the surgical staff there, he asked them to go over their instruments and pick out the fewest and most critical “for major operations in the front lines.” Continuing his research, he envisioned a25-bed portable hospital weighing 1,250 pounds that could be transported along jungle trails in packs and wheeled litters by four officers and 25 or 33 enlisted men, depending on how much other gear they had to carry.
Carroll formed 25 portables, as the units were called, by recruiting surgeons and medical technicians from big hospitals who were arriving from the United States. Carroll specified that all potential recruits had to be in shape. Because he felt that nurses would not be strong enough to carry the portable parts, he trained enlisted men to be surgical nurses. He eventually developed another version of the portable—larger and carried on trucks—that did include nurses. In their combat debut during the New Guinea campaign, the portables proved their worth. During their first week of combat in the fall of1942, surgeons in one portable performed 67 major operations.
MacArthur endorsed the portables, which were assigned to every infantry division in his command and were soon in use by Allied forces in India, Burma, and China. In Burma, a medical report said, surgeons normally worked by flashlight at night, “since litter bearers usually brought in patients after dark” to evade Japanese snipers.
Shortly before the war ended, the Army Medical Department decreed that, although the portables had saved thousands of lives, “no future was envisioned” for them. Instead, the army turned to Dr. Michael E. DeBakey, a Tulane Medical School professor and pioneer in cardiac surgery who would later pave the way to open-heart surgery. DeBakey offered his skills to the army, rose to the rank of colonel, and became an adviser to the surgeon general. He and other highly skilled ex-civilians, often challenged official dogma, as they developed surgical teams that traveled by truck from large combat-zone hospitals to the front. Out of that came the idea for Mobile Army Surgical Hospitals—MASH.
Approved by the Medical Corps too late for World War II, MASH became its salvation when the Korean War ignited in June 1950. Stripped of doctors by a rapid postwar demobilization, the corps was unprepared for this new war. But it did have a small number of MASH units, and three of them were rushed to South Korea to accompany combat forces.
Each was a 60-bed mobile hospital whose staff ideally included six surgeons, 10 other officers with medical specialties, a dozen nurses, and 95 enlisted men. In that war of sudden battles, there were days and nights when the number of wounded soldiers surged, and the official table of MASH organization collapsed. As one historian noted, it was “not uncommon for dentists to give anesthesia, psychiatric residents to perform surgery, or radiologists to set fractures.”
In order to provide the Medical Corps with more physicians quickly, Congress passed the Doctors Draft Act. It exempted experienced physicians who had served in World War II while drafting young, inexperienced physicians. For some of them, the first patients of their medical careers were wounded soldiers lying on a folding operating table in a MASH tent. The career army officers in a MASH had to learn to cope with those temporary officers, who saw themselves as physicians aiding the wounded rather than officers serving in the army. That was succinctly immortalized in dialogue from the movie MASH, between an army captain and two MASH doctors. The captain asks, “What are you two hoodlums doing here?” and one of the doctors answers, “Ma’am, we are surgeons, and we are here to operate.”
Describing the real-life doctors who served in Korea with him, Captain H. Richard Hornberger, a Maine surgeon called to war, wrote, “A few flipped their lids, but most just raised hell.” Hornberger, in collaboration with a ghostwriter, wrote MASH: A Novel about Three Army Doctors, published in 1968 under the pen name Richard Hooker. The movie MASH came out two years later, followed in another two years by the television series M*A*S*H*. Its final episode in 1983 attracted the largest audience to that point in television history.
The last actual MASH in Korea was deactivated in 1997. During the Vietnam War, the MASH concept evolved into medics in helicopter ambulances. In a war with no trenches and no front line, helicopters brought wounded soldiers directly from battle to large stationary hospitals within the sprawling bases throughout South Vietnam. Still, the concept of MASH continued into the 21st century. The final MASH, the 212th, traced its origin to the 12th Evacuation Hospital founded in World War I. The 212th ended its service helping injured civilians, survivors of the devastating 2005 earthquake in Pakistan. The unit was absorbed into a larger combat support hospital in October 2006, and its equipment was donated to the Pakistani army. After the 212th’s colors were wrapped, an echo of the fictional MASH came with the announcement that there would be “a cake-cutting ceremony in the triage section.”
Thomas B. Allen is the author of Tories: Fighting for the King in America’s First Civil War and co-author, with Norman Polmar, of World War II: America at War 1941-1945.
[hr]
This article originally appeared in the Spring 2015 issue (Vol. 27, No. 3) of MHQ—The Quarterly Journal of Military History with the headline: Surgery in the Front Lines
Want to have the lavishly illustrated, premium-quality print edition of MHQ delivered directly to you four times a year? Subscribe now at special savings!
![]()