The colossal hospitalization numbers from the COVID-19 pandemic have, at various points, forced hospitals in the United States to make hard choices regarding who receives life-saving treatment and who does not. Especially in the pandemic’s early days, public health officials took steps to establish triage guidelines for hospitals to follow should the number of critically ill patients outweigh, for example, the number of available ventilators. While the guidelines vary by state, they have one common thread: giving priority to those who are most likely to recover if given treatment.
The term “triage” is derived from the French word “trier,” meaning “to sort.” Triage has been practiced in the military at least since the Napoleonic era. Although triage was not used as a medical term until World War I, it was integral to the Civil War–era advancements made by Dr. Jonathan Letterman—advancements that still influence us today.
At the outset of the Civil War, no organized system of medical care and evacuation existed. This changed on July 4, 1862, with the appointment of Major Jonathan Letterman as Medical Director for the Army of the Potomac. Letterman reorganized the Medical Corps and created a system of medical evacuation designed to care for wounded soldiers from the moment of injury through long-term recovery, which became known as the Letterman Plan. In March 1864, Congress implemented Letterman’s changes across the entire Union Army. They remain today a basis for modern EMS and military combat medicine.
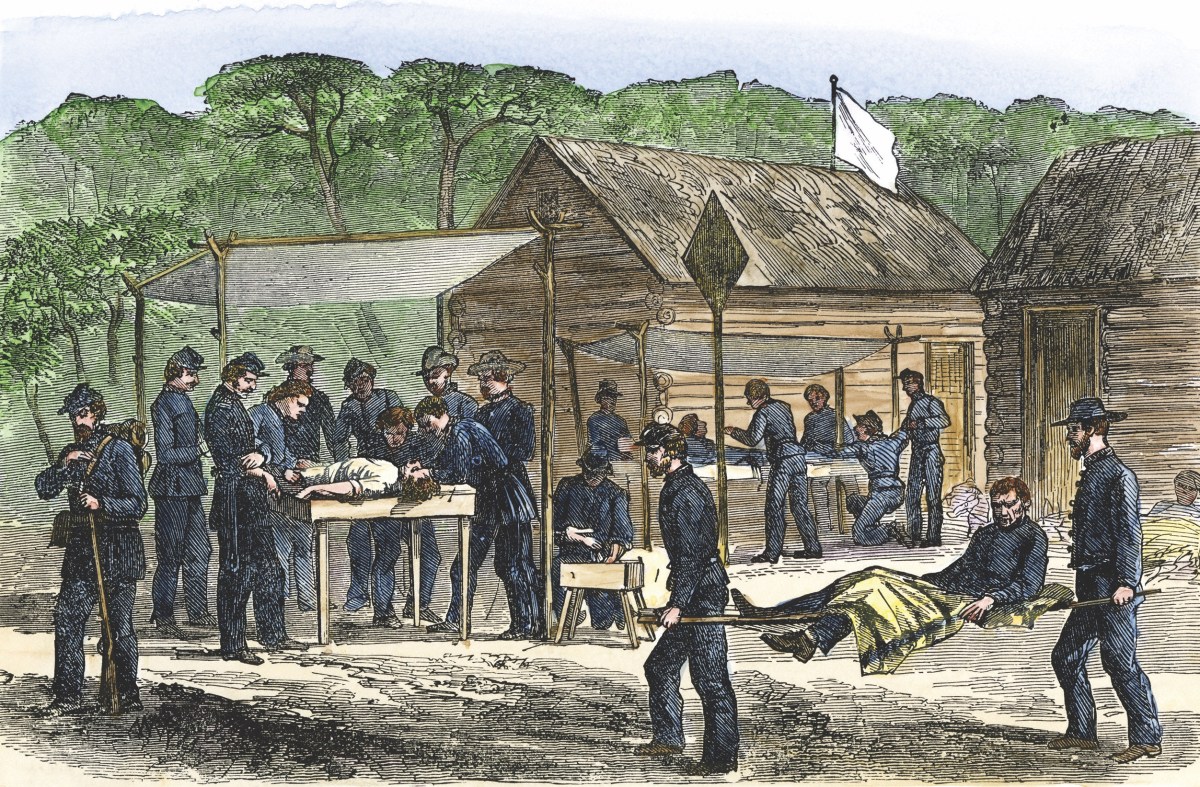
The first stop of Letterman’s plan was the field dressing station, located as close to the battlefield as possible. This is where triage was first performed. Here, the wounded were administered first aid and sorted according to the seriousness of their wounds. Patients were sorted using the following criteria: severe, mild, slight, and mortal. Severe wounds included serious bleeding, compound fractures, missing limbs, or major trauma to the arms and legs. These were taken by the ambulance corps to the nearest field hospital for immediate care. Mild wounds included excessive bleeding with the patient in stable condition and were evacuated after all the severely wounded were removed from the battlefield.

This article first appeared in America’s Civil War magazine
![]()
![]()
Slight wounds were minor enough to allow patients to be sent back to their units. Lowest priority were wounds that pierced the trunk of the body or head: what were normally mortal wounds. These patients were made as comfortable as possible and set aside until time allowed—not due to cruelty on the doctors’ part, but because they simply lacked the knowledge and technology to treat those kinds of wounds at the time. Such serious wounds weren’t necessarily a death sentence for soldiers. For example, there were about 200 reported cases of trephining (drilling a hole in the skull to relieve swelling in the brain or remove foreign objects like bullets or bone fragments), which had a 43 percent survival rate!
With the implementation of this system of triage, wounded soldiers were given a better chance of survival and went into battle knowing they would not be left on the battlefield for days waiting for help.
Modern triage closely mirrors its Civil War counterpart and is based on the principle of doing the greatest good for the greatest number with the available resources. While it is practiced throughout medicine by first responders and emergency room personnel, we usually think of triage in terms of mass casualty incidents, or incidents in which the number of casualties overwhelms medical personnel and resources.
In these instances, it is ideally performed rapidly, with 15–60 seconds spent categorizing each patient according to the colors red, yellow, green, and black. Red (immediate) patients are the first priority and include pneumothorax (collapsed lung), hemorrhagic shock (significant blood loss), closed head injury, and diminished mental capacity (unable to follow simple commands).

Yellow (delayed) patients have major or multiple bone, joint, back, and spine injuries with an unobstructed airway. Those placed in the green (minor) category are the “walking wounded”—those who can follow commands with minor cuts, bruises, painful and swollen deformities, and minor soft tissue injuries. The lowest priority is given to those who fall in the black (deceased) category. Examples of this category include undisputed mortality or death, such as decapitation, blunt traumatic cardiac arrest (no pulse or spontaneous respiration), injuries incompatible with life, and the existence of visible brain matter. Keep in mind that triage is to be an ongoing process that is performed continuously throughout the primary assessment, treatment, transportation, and hospital phases of care.
While medical care and knowledge of physiology today has far surpassed that of the 19th century, triage categories have remained largely unchanged since the Civil War. Our modern red, yellow, green, and black triage categories all closely mirror the Civil War-era categories of severe, mild, slight, and mortal wounds. In both cases, red (severe) always receives the first priority. Yellow (mild) is next, green (slightly) third, and then black (mortal wounds) last.
The current COVID-19 pandemic is the latest tragic example of modern-day mass casualty events that highlight how the innovations of Civil War medicine continue to benefit us. The measures taken by the medical community in response to the pandemic showcase the evolving nature of triage and the ability of medical personnel to adapt to these changing circumstances. Thanks to Dr. Letterman and the advancements made in medical evacuation during the Civil War, medical personnel have the framework they need to use available resources to save the greatest number of lives. As our world struggles to deal with a deadly pandemic, the changes wrought during the Civil War remain just as pertinent, if not more so, today.