Better fall back a few yards,’ said the officer, and even as we were doing so something jabbed my hand. It dropped down and blood spurted out. The others had gone. I was alone….From the pillbox, hidden somewhere about…a couple of bits of lead whistled. I crawled into an enormous shell hole and began to sink into mud. With the slime clinging to me I got away, through the bottom of a hedge which, by the grace of God, had remained there. No one to be seen now and my head facing I knew not where….Not far away a tank, half embedded, was getting it full tilt. The sweat stood on my dirty face. And then in that great expanse of mud and wire I spotted a little red cross on a little flag, sticking eighteen inches out of the ground. I felt safe again.’
Private Alfred Willcox, Royal Sussex Regiment, was just one of the 310,000 casualties sustained by the British Expeditionary Force (BEF) during the Third Battle of Ypres, a controversial campaign that dragged on from July 1917 until Passchendaele fell to the Allies in November. For Willcox and millions like him, the ‘little red cross on a little flag’ meant the difference between life and death. It was the emblem of the medical corps — the stretcher-bearers, orderlies, doctors, nurses and many others who often risked their own lives to care for the wounded.
Medical treatment for battle injuries is as old as warfare itself. It is discussed in ancient Egyptian surgical texts from 3000 bc. Greek physician Hippocrates (ca. 460-377 bc), for whom the doctor’s Hippocratic Oath is named, advised his disciples, ‘He who would become a surgeon, let him join an army and follow it.’
Humanitarian considerations aside, the need to conserve trained fighting men by caring for their wounds has made sense for millennia, but treating those casualties on the front lines is a relatively recent development. In the West, Queen Isabella is usually credited with the creation of field hospitals; during the reconquest of Spain from Muslim rule in the 1480s she provided medical tents for her wounded soldiers. (Given that Islamic medicine at the time was greatly advanced compared to that of Europe, some have suggested that Isabella got the idea from the Moors.) The use of military hospitals and even mobile field hospitals caught on slowly. The English, for example, did not establish field hospitals until King William III’s bloody trek through Ireland in 1690.
Modern military medical practice owes much to Napoleon Bonaparte’s chief surgeon, Dominique Jean Larrey. Larrey’s greatest contribution was the flying ambulance — a horse-drawn wagon that evacuated wounded from the battlefield, so that they could be tended to farther behind the lines. His use of triage — treating the wounded according to the severity of their injuries instead of by rank — was considered quite radical at the time; today it is standard operating procedure. Larrey was also a proponent of immediately amputating a damaged limb rather than waiting until it became gangrenous, at which point it was usually far too late to save the limb or the life.
Military medical care followed the same pattern for more than a century. Stretcher-bearers would remove the wounded from the field and take them to a dressing station located just out of range of enemy small-arms fire and equipped with the barest essentials. In the American Civil War, for example, that included bandages, chloroform (if it was available), morphine, opium and whiskey. The surgeon’s task was to stop the bleeding and prevent shock until the wounded troops could be moved farther behind the lines for treatment in a field hospital. Over time, this basic method of evacuating the wounded and providing care developed into a remarkably efficient system.
In the early 1900s, the Medical Department of the U.S. Army and the British army’s Royal Army Medical Corps (RAMC) were probably the best-prepared military medical outfits in the world. Both armies had learned harsh lessons about the importance of quality medical care during the Spanish-American and Anglo-Boer wars, in which the Americans and the British respectively lost more soldiers to typhoid than to combat. They entered the 20th century determined to attract quality medical professionals to military service and to enforce basic hygiene and other preventive measures among the troops. Nothing, however, could prepare them for the catastrophe that awaited as the world rushed headlong toward 1914.
World War I produced horrors the likes of which had never been seen. Some 65 million troops were mobilized by the Allies and Central Powers; more than 37 million — approximately 57 percent — were counted among the dead, wounded or missing at war’s end. Treating those casualties was a gargantuan task, and the work of the RAMC serves as a good example of life on the Western Front.
The RAMC established three working zones: the collecting zone (that closest to the battlefield where the wounded were taken first); the evacuating zone (located along lines of communication with vehicles to transport the wounded to the rear); and the distributing zone (the location of more permanent structures such as base hospitals).
The regimental medical officer (MO) was the first crucial link in this chain. His aid post was situated within yards of the main fighting trench, but if the fighting — or wound — was such that a soldier could not be moved, the MO attended casualties in the trench itself. Fighting trenches measured approximately 2 feet wide at the bottom, 4 feet wide at the top and 6 feet deep. Fire-steps were dug into trench walls about a foot off the ground where stretchers could be placed out of the way of fighting men. In waterlogged trenches, which were common, the fire-step also kept the wounded dry.
The cramped quarters made maneuvering stretchers difficult, to say the least; sometimes they had to be carried over open ground. Generally these removals took place under cover of darkness unless the nature of the wound was so critical that the soldier had to be moved under fire at whatever cost to the stretcher-bearers and the soldier himself. (Stretcher-bearers suffered extremely high casualty rates, and the RAMC is the only component in the British army to have had two members awarded double Victoria Crosses.)
At the regimental aid post, the first priority was to keep a wounded soldier warm and to prevent shock. His wounds were cleaned and bandages applied. Broken limbs were splinted. The patient might also be given a tetanus shot, as there was always the risk of infection. Dead tissue was cut away when the wound was cleaned, and the MO had to be extremely careful to remove any bits of clothing or other foreign matter that could turn a wound septic. Then the soldier would be made as comfortable as possible until a field ambulance could transfer him to a dressing station. Private Willcox was one of the walking wounded, a soldier who could get to the dressing station under his own steam. He might as well have found himself in a different universe: ‘In the early hours of the morning I tumbled into an electrically lighted dug-out dressing station two miles from the front line where there were clean bandages and steaming tea. I fell at full length, motionless. Someone pressed drink to my lips.’
Triage was carried out at the dressing station, and the wounded were separated into three categories: those with less serious wounds that could be dressed and then sent on to the field hospital for further treatment; those requiring immediate emergency treatment; and the ‘hopeless cases’ who were given palliative care, often in the form of morphine or chloroform.
The field hospitals — or casualty clearing stations in the RAMC — were, in the words of a 1917 British Medical Association manual, ‘real hospitals, despite the fact that some are only about six miles from the fighting line….The patients are nursed by trained women nurses; ordinary hospital beds are provided for the most severe cases; the operating theatres have usually four operating tables…electric light…and some have X-ray annexes of their own….[C]linical laboratory work is done for them by the mobile laboratories….’
Casualty clearing stations (CCS) had the amenities of civilian hospitals, but the comparison ended there. Dr. John Hayward had 20 years’ experience as a general practitioner and served a brief stint at a Red Cross hospital in England when he volunteered to go to France in 1918. Assigned as a surgeon to the CCS at Amiens, he was overwhelmed at first by the volume and the difficulty of the work:
They come in such numbers that the tent is soon filled. Many are white and cold, and lie still and make no response, and those who do are laconic….I have had no instructions how to dispose of such numbers, or the method of procedure, but realize that they must be examined briefly and sorted, and sent to one or other of our hospital tents….It was 7 a.m. before I had cleared the tent…but at 10 a.m. I should have to begin to operate for another twelve hours and on cases like these!
It was extraordinary that in this charnel tent of pain and misery there was silence, and no outward expression of moans or groans or complaints. The badly shocked had passed beyond it; others appeared numbed, or too tired to complain, or so exhausted that they slept as they stood….
`Resuss’ [resuscitation tent] was a dreadful place. Here were sent the shocked and collapsed and dying cases, not able to stand as yet an operation, but which might be possible after the warming-up under cradles in heated beds or transfusion of blood. The effect of transfusion was in some cases miraculous. I have seen men already like corpses, blanched and collapsed, pulseless and with just perceptible breathing, within two hours of transfusion sitting up in bed smoking, and exchanging jokes before they went to the operating table….
That dreadful day of my first experience of a C.C.S. rush ended…after thirty-six hours of continuous work, and somehow I had got through. I was completely exhausted with anxiety and fatigue, and felt I could never go on with it, and was not up to the task: but to give in was even more terrible.
That dreadful day of my first experience of a C.C.S. rush ended…after thirty-six hours of continuous work, and somehow I had got through. I was completely exhausted with anxiety and fatigue, and felt I could never go on with it, and was not up to the task: but to give in was even more terrible.
The ambulance drivers who transported the wounded in a steady flow from the aid post to the dressing station to the field hospital had their share of harrowing experiences. Speed was essential, but so was remembering that severely wounded men could not stand to be bounced around over roads pitted by countless bombardments. There were other hazards, too, as Leslie Buswell, an American volunteer, recalled in American Ambulance Field Service in France:
About ten o’clock I had a call to go to Auberge St. Pierre for two seriously wounded, and when I arrived there, the mdecin chef told me that if I got them to the hospital quickly, they would have a chance of living. So ‘No. 10’ tooted off down the hill — at what the plain warrior would term — ‘a hell of a pace….'[O]n turning to go to Dieulouard where we take the wounded I saw a huge shell explode two hundred metres down the road I was to drive along. Had the ambulance been empty, or with only slightly wounded, I should have waited, of course, but under the circumstances my duty was to go on as fast as I could. I noticed ahead of me three large motor-trucks and the thought struck me: ‘What if those are hit and contain ammunition.’ I was ten yards away when — bang! — I was half blown out of my seat — a shell had landed on the motor-truck. Hardly believing I was not hit, I increased my pace and emerged from the smoke and blackness, going at a good clip, safe and sound, but shaken….[W]hen I arrived at Dieulouard, I noticed that everybody was pointing at my car. I supposed it was because we looked so smoke-grimed….I then got down to discover what was troubling them. One of the poor fellows had thrown himself off the stretcher and all of his bandages had slipped and a trail of red was flowing from the car and leaving a pool on the ground.
Medical personnel also had to contend with more efficient — and therefore more deadly — weapons. Flamethrowers were introduced by the Germans and quickly adopted by the Allied forces. One automatic machine gun was reckoned to have the same firepower as 80 rifles. But perhaps nothing was as devastating as chemical warfare. The French first used tear gas in battle in 1914, but the Germans were the first to use a lethal agent when they launched an attack with chlorine gas in April 1915, at the Second Battle of Ypres. Harder to detect and potentially more dangerous than chlorine was mustard gas. Practically odorless, it had no immediate effects, but within hours of exposure, the gas caused severe internal and external blisters. It also contaminated the soil for weeks after its release. Steps were quickly taken to protect soldiers from gas attacks, and by the war’s end, both sides employed highly effective respirators with charcoal filters — a definite step forward from holding cotton pads dipped in a solution of bicarbonate of soda or urine-soaked cloths over the face. It was just another chapter in constantly evolving warfare.
The battlefields of World War I laid the foundations for the medical advances that were to follow in World War II, Korea and Vietnam. War has always served as a proving ground for medical techniques that were later adapted to future military and civilian use.
Among the most important developments during World War I were improvements in blood transfusions and the diagnostic use of X-rays. For the first time, the military addressed the psychological effects of war, as’shell shock’ accounted for a considerable number of casualties. The widespread use of reconstructive surgery, orthopedic surgery and physical rehabilitation marked a turning point in preparing the veteran for postwar life.
By the end of the war, it was well understood that the sooner a wounded soldier received treatment, the better his chances of survival. Aid posts in the trenches and motorized ambulances were a boon, but as the pace of life in general accelerated in the run-up to World War II, so did the means by which the military dealt with its wounded. Combat medics were incorporated into fighting units and went into battle to administer immediate care in the field under fire. Like the stretcher-bearers in World War I, combat medics suffered high casualty rates.
World War II also ushered in the era of sulfa drugs and penicillin to treat infections. The synthetic antimalarial drug Atabrine was used extensively in the Pacific after the Japanese occupation of the Dutch East Indies effectively cut off the quinine supply. A method to separate plasma from whole blood was perfected in the 1930s, giving field medics a viable option for stabilizing the wounded when whole blood was unavailable. Morphine, which had been used in field hospitals for decades, was now available in individual doses that could be injected immediately, bringing a measure of comfort until the wounded could be evacuated from the field. Thanks to this progress, in World War II only 4.4 percent of those wounded died, compared to 8.1 percent in World War I.
Mobility was the watchword of the post-World War II era. The U.S. Army experimented with various mobile medical facilities before adopting the mobile army surgical hospital (MASH) late in 1945. Used extensively for the first time in Korea, MASH units were designed to move in response to the fighting. The first three MASH units — 8055th, 8063rd and 8076th — moved 50 times between July and December 1950; the 8076th alone admitted more than 5,000 patients as the battle for the Pusan perimeter raged from July to September.
What made this all possible was aeromedical evacuation, perhaps the most significant technological development in 20th-century military medicine. World War I saw the limited use of airplanes to move the wounded, but the field progressed rapidly. In World War II, the U.S. Army Air Forces modified a Douglas C-47 to carry 18 patients on stretchers in addition to medical technicians and nurses.
Arguably the most revolutionary development was the medical evacuation, or medevac, helicopter, which became symbolic of the Korean and Vietnam wars. In terrain that was often inaccessible to ground transport, the medevac could carry surgeons into the field if necessary, as well as carry wounded out. By 1951, 60 to 80 percent of battle casualties were taken to field hospitals or other treatment facilities the same day they were wounded. In Vietnam it was possible for a wounded soldier to reach a hospital within two hours. It was a far cry from World War I, the first industrialized war, when the journey from the trenches to the field hospital could take between 12 and 48 hours.
More than 50 years after Private Willcox stumbled into a dressing station in Ypres, Sergeant Fred Castleberry lay on a battlefield halfway around the world near Trang Bang, Vietnam. It was April 14, 1968 — Castleberry’s 21st birthday — and a rocket-propelled grenade had just severed his right arm below the elbow and his left leg above the knee.
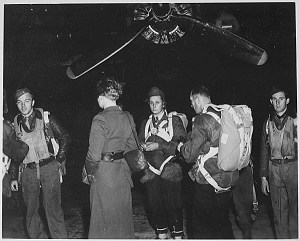
Castleberry was doubting that he’d ever make 22 when he saw a ‘big green angel,’ a Bell UH-1 ‘Huey’ helicopter bearing a red cross — the officially recognized symbol of the medical corps since the 1864 Geneva Convention — coming for him:
For the rest of my life, I will never forget the whopping sound of the Huey’s blades and the sight of the spotlight clearing the tree line. As the Huey got closer, I could see sparks flying everywhere, as countless small-arms rounds hit the helicopter….I honestly thought the helicopter would be shot down, and we would all die.But somehow, through all of the gunfire, they got in. I remember seeing these beautiful angels pick me up and take me aboard. I remember the pinging of the bullets ripping through the skin of the Huey and hearing the crew excitedly, yet calmly, talking to one another. Then I saw this face above me saying, ‘Buddy, stay with me. Hey, Buddy, you are going to be all right.’ Over and over again I would drift in and out of consciousness, and all I can recall is this bloody face telling me I was going to make it.
When I came to, this nurse asked me if I would like company….The entire dustoff crew was in the hospital with me. The guys that saved my life, the young boys that rescued me themselves had been wounded. The blood on the air medic’s face was not mine; it was his. A bullet had gone through his cheek, and rather than tend to his own wounds, he kept me alive.
Castleberry testified before the U.S. Senate Committee on Veterans’ Affairs in July 2003 during a hearing to determine whether the criteria for awarding a Combat Medical Badge should be changed. Established in 1945, before the age of helicopters, the CMB has been given to ground personnel who provided medical aid in combat.
A bill to create a Combat Medevac Badge to recognize helicopter pilots and crews passed the U.S. House of Representatives in May 2005. As of June 6, it had been referred to the Senate Armed Services Committee.
This article was written by Christine M. Kreiserand originally published in the November 2005 issue of Military History magazine.
For more great articles be sure to subscribe to Military History magazine today!