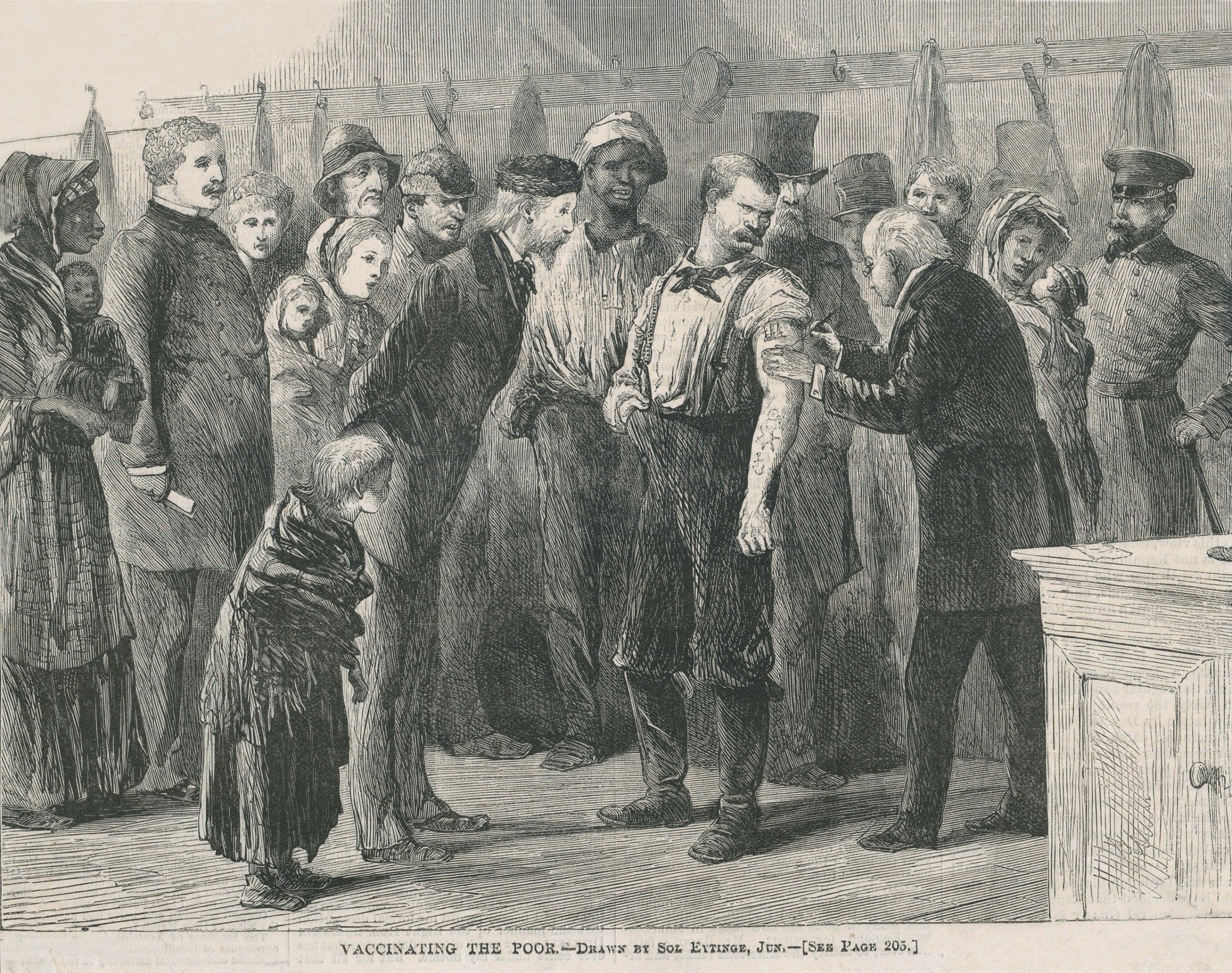
Vaccination efforts became standard for both armies desperate to prevent the spread of deadly smallpox
The soldiers mostly carried Springfield, Enfield, or Lorenz rifled muskets rather than M4 carbines, wore blue or gray rather than green or tan combat uniforms, and they might have seen balloons flying overhead rather than drones, but among American forces, one similarity between military life in the Civil War and today was in a simple requirement: Get vaccinated.
COVID-19 was far in the future; the requirement was for the smallpox vaccine. At the time, vaccination was relatively new and viruses, such as the one that causes smallpox, wouldn’t be discovered for 30 more years and wouldn’t be seen by the human eye until after the first electron microscope was built in the 1930s.
The first vaccine was developed in 1798 by Edward Jenner, an English country doctor, and it was against smallpox. Preventive measures of vaccination and isolation had drastically reduced the occurrence of the disease in the early to mid-19th century, but by the 1840s, Americans were beginning to neglect vaccination, and there was a generation that had never been exposed to the disease. As a result, the incidence of smallpox began to rise in the decades before the Civil War.
From May 1861 to June 1866, 12,236 cases of smallpox were reported among White troops in the U.S. Army (5.5 per 1,000 men annually) and 6,716 among U.S. Colored Troops (36.6 per 1,000 men annually). For White troops, the death rate from the disease was approximately 23 percent; 35 percent for Black troops. The prevalence of vaccines meant that while smallpox stacked up among the deadliest diseases of the Civil War, it was not among the most common, ranking among the least-frequent diseases for White soldiers and middle of the pack for Black troops. That Black soldiers suffered a higher mortality rate from smallpox (and most other diseases) likely demonstrated the impact on their nutrition and health from being enslaved—a recent factor for many.

Prior to the development of vaccination, another form of inoculation—variolation—was used to combat smallpox. That treatment is the introduction of disease agents into the body to produce a mild form of the disease—usually by using pus or scabs from infected persons and administering them to the patient through small cuts made in the skin. It was intended to confer immunity by producing a mild case of the disease. Unfortunately, not all cases were mild, and deaths were associated with the treatment, though at a far lesser rate than among those naturally acquiring the disease. Variolation was in widespread use as early as the 1720s and, despite the danger, continued to be widely practiced throughout the 18th century.
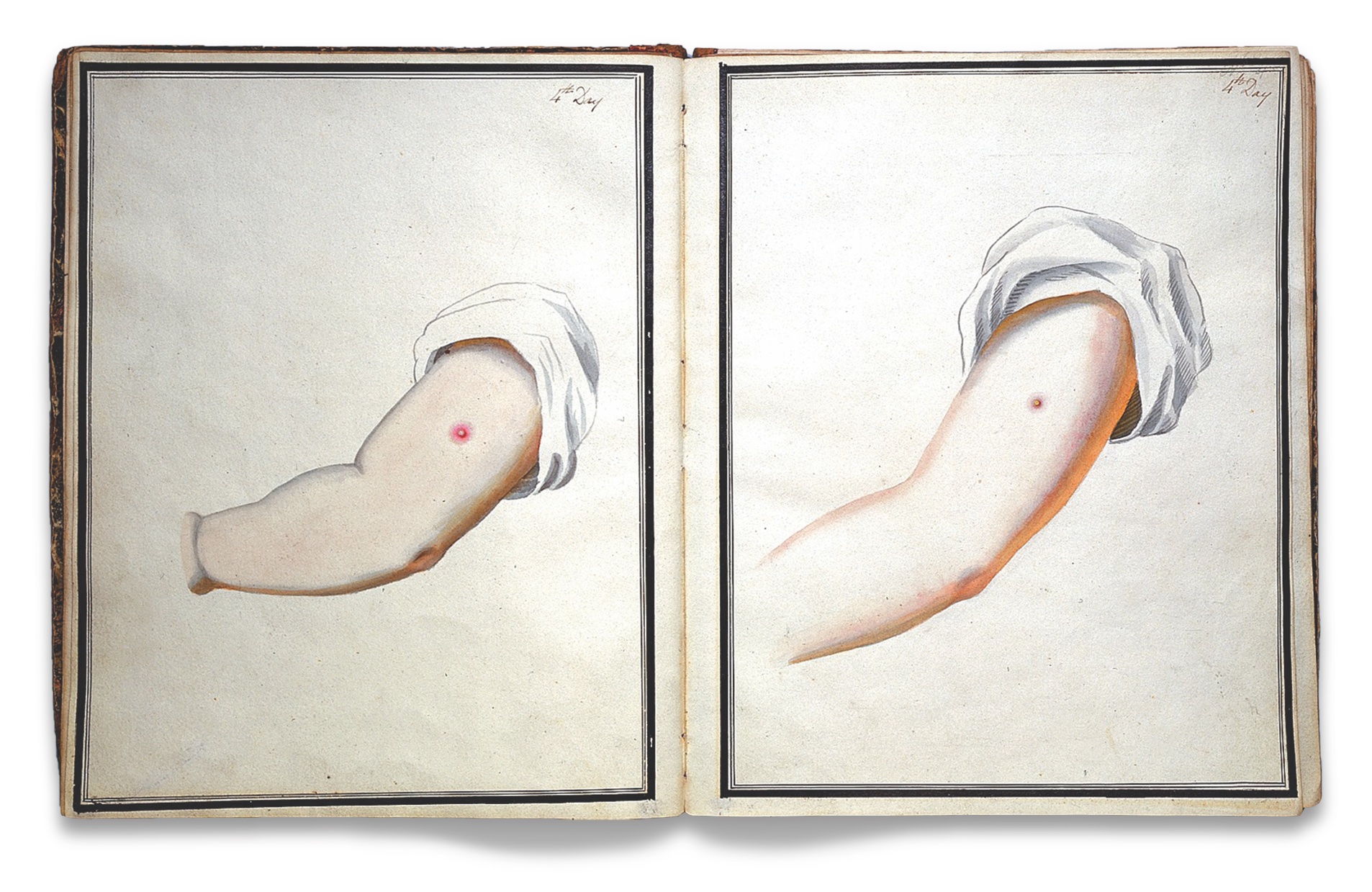
Jenner’s breakthrough was to use cowpox serum. Cowpox, a closely related disease, is rarely fatal to humans, but it created a resistance to smallpox. As with variolation, the vaccine was administered through a series of small cuts in the skin, usually in the arm. The cowpox virus was obtained from animals infected with cowpox. By the 1830s, vaccination was widely accepted, especially among physicians. Variolation was still practiced in some places until it was outlawed by individual states. The bans were based on the fear of spreading the disease through inoculated persons since they were infectious, unlike vaccinated persons. By the outbreak of the Civil War, variolation was illegal in most places, but still occasionally practiced.
Quarantine, vaccination, and the destruction of infected clothes and bedding were the primary tools used to control smallpox’s spread in the armies during the war. Most hospitals had a separate ward, or even a separate facility, in which to isolate smallpox patients because of the disease’s well-known contagiousness.
Both Union and Confederate regulations required the vaccination, and re-vaccination if necessary, of all troops. However, many soldiers weren’t vaccinated because most regiments were raised by the individual states and the regulation was disregarded in the rush to send large numbers of men into battle. Since there had been no systemic vaccination of the civilian populations, many of the recruits had never been vaccinated or exposed to smallpox. For those who were vaccinated, re-vaccination was recommended after seven years—or when men were directly exposed to the disease.
The best and purest source for the vaccine was from cows or calves. The crust from the cowpox pustules was used as the source for the inoculation, though in at least one instance, crusts came from calves infected with the “humanized” virus, not naturally occurring cowpox. The pressing demands of war often led authorities to institute programs that obtained the scabs from vaccinated humans. The Union medical dispensaries of the Northern cities supplied vaccine virus in the form of crusts taken from vaccinated infants, each with a certificate listing the dispensary and the child’s name. In the Confederacy, many programs were set up to ensure an adequate supply of vaccine scabs for the Army. Every hospital had a medical officer whose job was to search the surrounding populace for children in whom they could propagate cowpox. Ads were taken out in local newspapers offering free vaccination to children if the crusts were then allowed to be harvested. Both White and African American children were used to supply scabs, and in at least one instance, a small group of African American children were kept vaccinated to provide usable material. The children were vaccinated in six places in each arm. In two weeks, the crusts were removed, wrapped in tin foil, and shipped to army surgeons. Late in the war, a shortage of virus material led to an authorization to pay private physicians $5 per usable scab.
Children and cows were the safest sources for crusts, but other methods were used as well. Surgeons often used the scabs from recently vaccinated men to vaccinate other soldiers. Soldiers did the same among themselves, sharing the crusts and using knives to make the incisions in their arms. Some men even sent scabs home for the use of their families. In most of these cases, guidelines involving the appearance of the scab and the proper number of days to wait to harvest the crusts after the initial vaccination were not followed.
Unfavorable results from vaccination, or spurious vaccinations, were all too common. Even pure vaccine, obtained from official Army dispensaries, sometimes caused complications. Sometimes, faulty preservation of the crusts could have compromised their effectiveness. As is the case even with modern vaccines today, occasionally, the vaccine did not take, failing to produce the major reaction at the vaccination site that was expected. In other cases, the site of the vaccination became overly sore and swollen, and abnormal pustules developed, leaving surgeons to question whether those vaccinations had been effective.
Complications from using a scab from a recently vaccinated adult were even more deleterious. Since many vaccinations took place in hospitals, crusts from men who were sick with other conditions were occasionally used unintentionally, spreading disease rather than preventing it. Often, soldiers in a hospital or prison didn’t get vaccinated until smallpox had already appeared in the facility, increasing the risks for some who might not have otherwise been exposed to the disease.
Perhaps the worst, and unfortunately common, form of spurious vaccination was the use of scabs that were syphilitic in nature. This occurred both in the hospitals and among the soldiers who self-vaccinated. Misdiagnosing a scab or harvesting crusts from the arm of a soldier who had syphilis would spread this disease to everyone vaccinated from that source. In one notable case, two brigades were affected by a vaccination infection that was thought to be syphilitic in nature. The men were so sick that the brigades were unfit for military service. The epidemic was traced to a single soldier who had obtained vaccination material from a woman who likely had syphilis.
The Confederate Medical Department attempted to prohibit soldier-to-soldier vaccination to limit these damaging effects. Even civilians were discouraged from self-vaccination, as the consequences of spurious vaccine had spread to the general population as well, leading to a mistrust of the vaccination process.
Research into the history of smallpox vaccinations led to the discovery that the actual virus used in vaccinations was the vaccinia virus, of the same family as the smallpox (variola) and cowpox viruses, but genetically distinct. The origins of the vaccinia virus are unknown, but it is believed to have originated in the 19th century.
The preventive measures of vaccination and isolation taken by the Union and Confederate medical departments curbed the occurrence of smallpox during the war and averted any major outbreaks. The success of the vaccination of soldiers during the war led to widespread postbellum vaccination of the civilian population, further helping to control this serious disease.
Terry Reimer is director of research at the National Museum of Civil War Medicine in Frederick, Md. She has more than 20 years of experience in historical archaeology and research, specializing in 17th-, 18th- and 19th-century American sites.